Muslim girls of East Bengali descent living in the Chars and the Kaivartta fisherfolk are suffering due to early marriage and childbirth
Tutu Begum was just 15 when she was married to a man five years older to her. A year later, she delivered a baby girl. Now 22, Tutu is a divorced mother living with her parents and daughter, who is enrolled in a primary school near their rented house in Assam’s North Lakhimpur town. Tutu belongs to a community of Muslims of East Bengali descent which, according to a socio-economic survey done by the Directorate of Char Development in 2001-02, is among the most backward in Assam.

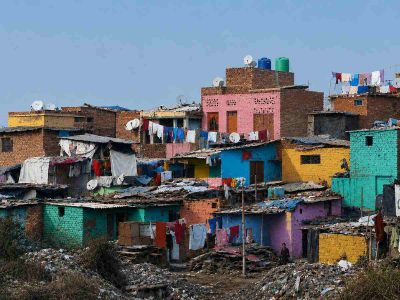
The community is concentrated largely in Lower and Central Assam villages set in riverine areas called the Chars. Its members have for long been falsely demonised as “illegal Bangladeshi immigrants” and, as a consequence, have suffered discrimination. The community has among the highest rates of child marriage and childbirth in Assam. And women and girls have been bearing the brunt.
Tutu’s parents are originally from Lahorighat in Morigaon district of Central Assam. They lost their agricultural land to erosion by the Brahmaputra river and left to work as farm labourers in Nagaland before settling in North Lakhimpur. Her father earns a living pushing a handcart, while her mother does domestic chores at several homes in the town. Tutu has three brothers, all of whom were married in their early 20s to adolescent girls.
Since there’s a preference for boys, women end up having several daughters in the hope of finally bearing a male child. One consequence is that the rate of maternal mortality is quite high, another is that polygamy is not uncommon. Women, thus, have little control over their lives. When Tutu’s husband divorced her — he suddenly started disliking her and asked to separate, she says — she had no choice but to return to her parents, her young daughter in tow. Her family is keen for her to remarry but Tutu is reluctant because marrying again would mean bearing more children — and she doesn’t want that.
Rahela Begum, 25, a daily wage worker in North Lakhimpur town, has a similar story. Married at 15, she’s mother to a nine-year-old and a six-year-old. A severely anaemic Rahela is struggling to raise her children alone. Her mason husband works in Arunachal Pradesh, where she fears he may have another wife and children. She’s afraid of confronting her husband, though, or informing her in-laws, lest it ends up in separation.
Safika Khatoon was 17 when she died giving birth to her second child in a year. Complications first developed during the sixth month of her pregnancy, recalls her mother Sarifa, 35, who too was married and bore children in her adolescence. “She had severe headaches and abdominal pain for which we took her to a gynae-cologist,” Sarifa says of her daughter. “The doctor said Safika had high blood pressure.”
She was put on medication but required an emergency delivery after eight and a half months of pregnancy. She didn’t survive the delivery, nor did her baby.
Aside from poverty, a key reason for this state of affairs is a lack of access to quality education and healthcare. Tutu, for one, did not even finish primary school because her family wanted her to be “ready for marriage” by training her in household work. Moreover, the community is largely reluctant to send girls to high schools outside their villages because “it may expose their modesty”. Most of those who do go to high school are wed before they finish class 10 as the community generally considers 15-16 to be marriageable age for girls.
Rahela studied up to class 6 in her Panbari village, around 30 km from where she now stays in North Lakhimpur town. She, however, attended the morning school attached to the village mosque where she learned enough Arabic to read Islamic scriptures. Many of the children from the community who go to these morning schools later join madrassas, which teach the Quran, classical Arabic and Islamic jurisprudence. Although most of the madrassas are for boys alone, there are some for girls too.
The lack of education means that girls are often left to cope with the issues of marriage, pregnancy and childbirth quite early, and struggle to live a life of equality and dignity. Both Tutu and Rahela are unskilled young women who struggle to find work in a small town with limited opportunities. Despite the provision of free midday meals, uniforms and textbooks at the primary level, and cycles for girls at the secondary level, the state’s education system still doesn’t attract a large number of girls from this community. A key reason is the community’s indifference towards girls’ education.
Rahela has been experiencing painful periods and bleeding in between since her husband started visiting her regularly from Arunachal last year. Her symptoms indicate she may have Chlamydia, one of the most common sexually transmitted diseases that can cause permanent damage to the woman’s reproductive system and even potentially fatal ectopic pregnancy (pregnancy that develops outside the womb).
She saw an OPD doctor at the North Lakhimpur Civil Hospital who prescribed some medicines and advised her to take a vaginal swab test. Since the facility for the test isn’t available at the hospital, Rahela was told to go to a private clinic. She can’t afford to pay Rs 400 for the test, however, and is reluctant to ask her husband.
In Rahela’s community, adolescent mothers are increasingly exposed to promiscuous husbands who work in distant places, including Arunachal, Kerala, Tamil Nadu, and Andhra Pradesh.
They are also at risk to reproductive health problems. An enquiry into Safika’s death later found that she suffered from preeclampsia, a condition in which a pregnant woman who has a history of normal blood pressure develop high blood pressure. Preeclamptic women have high levels of protein in urine and, often, swelling in the feet, legs and hands. It can impair kidney and liver function, and cause blood clotting problems, pulmonary edema (fluid in the lungs), seizures. In severe cases or when left untreated, preeclampsia can cause maternal and infant death. Preeclampsia reduces the blood flow to the placenta, often leading to smaller or prematurely born babies, as is quite common in this community.
Tutu does not have major sexual and reproductive health concerns but she has other health problems. Of late, she is developing pale white patches on her lower face, neck and back. She too saw a doctor at the North Lakhimpur Civil Hospital who prescribed an ointment to apply on the affected areas and Vitamin E capsules. White spots or patches on skin are usually caused by deficiencies of calcium, and Vitamins D and E. Having a balanced diet is essential for treating these nutritional deficiencies. But for Tutu, who lives in a cramped house with her parents and young daughter, a balanced diet is a luxury.
Safika’s death indicates the lack of proper healthcare services for the marginalised community. Though more and more women are having institutional deliveries, a substantial number still deliver at home. That’s mainly because gynaecologists are rare, especially in rural areas. At many Primary Health Centres, the government has appointed Ayurveda doctors who attend to pregnant women and administer labour.
Assam started two health schemes targeted at pregnant women a decade ago but both have since been terminated. Majoni, launched in February 2009, gave a pregnant woman Rs 500 each to undergo two health checkups at a government hospital as well as a fixed deposit of Rs 5,000 if she has a girl child. Mamoni, started the same year, encouraged pregnant women to undergo at least three antenatal checkups by offering them Rs 500 each after second and third checkups. The money was supposed to pay for nutritional food and supplements. But in most cases, they spent it to meet household needs.
Anima Das, 24, of Kolakhowa village in Dhemaji district was married six years ago, when she was still in school. She gave birth before she was 18. She got pregnant again but went for an abortion after around a month and a half at the instance of her husband and his family who did not want another child so soon. Her husband bought pills from a local chemist and she took them. The result was disastrous. Anima started bleeding profusely. Instead of taking her to the hospital, her family brought some paste of herbs from a village healer. Though her bleeding stopped, Anima has been unable to conceive since.
Anima is from the Kaivartta fisherfolk community, which is listed as a Scheduled Caste. The Kaivartta differ from the Muslims of East Bengali descent linguistically and religiously, and mostly inhabit river banks. They are among the most backward communities in Assam, with high poverty, low education and employment rates, and poor health. They are also socially marginalised on the basis of their caste.
Among the Kaivarttas too, girls are married young and often bear children in their adolescence. And young women often use unsafe methods for abortion due to the social stigma attached to it; they take pills bought over the counter or some herbal medicine prepared by a local practitioner. Sometimes, anecdotal evidence suggests, this proves fatal.
Jina Das, 23, had an abortion done by an untrained nurse in a chemist’s shop 10 km from her home in Adisuti village of Majuli district. She got married when she was 17 and gave birth a year later. The abortion, involving a painful procedure without safety measures, rid Jina of an unwanted second pregnancy. But it damaged her health. She now looks middle-aged, with a pale face and weak body. Before her marriage, Jina had developed a vaginal infection as girls in the community are required to sleep on a mud floor during their periods.
Poverty and the lack of decent healthcare for her community means Jina is unlikely to recover her health.
This ground report has been produced as part of the TMR 2019 Fellowship, an initiative by The Media Rumble to facilitate exchange of ideas between journalists and media houses from across India. The fellowship is supported by the Population Fund of India
www.newslaundry.com